Patellar Tendon Autograft
History of Using Patellar Tendon Autograft in ACL Surgery
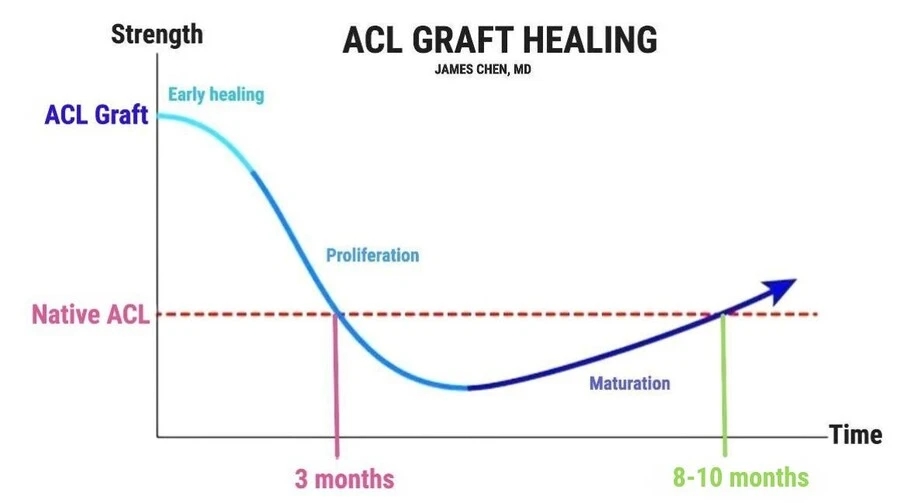
The patellar tendon is also known as a BTB (bone-tendon-bone) graft due to the patella bone and tibial bone blocks on each side of the tendon. The patellar tendon graft has a long tradition of being a solid ACL graft. Originally it was a preferred graft because it was thought that the bone on either end would heal into the bone tunnels by two months and therefore allow a quicker return to sports. It was later discovered that ACL graft healing takes 10 to 12 months to fully revascularize the graft. Thus, there is no advantage to having bone plugs with respect to a quicker return to sports.
What are the advantages of patellar tendon grafts?
The patellar tendon has a long history of being the gold standard graft in contact athletes such as professional football and rugby players. Multiple large studies show a very low re-rupture rate with these grafts. The graft itself is usually a 1 cm diameter graft. It can be larger or smaller according to the surgeon’s preference for graft size. The graft has a bone block on either side taken from the patella and tibia. The bone blocks fit into the drilled bone tunnels. One mechanical advantage of the BTB graft is that each bone plug is fixated with a screw and screw fixation is very strong.
What are some disadvantages of patellar tendon grafts?
The incision is typically linear about 4 to 7 cm so this harvest has a longer scar compared to other grafts. About 30% of patients have pain when they kneel on their scar. The patellar tendon graft is usually 1 cm in diameter. On average, the patellar tendon is 3 cm wide. Therefore, the harvest will take one-third of the native tendon. Theoretically, losing one-third of the patella tendon could affect the function in a kicker or jumper. Additionally, some studies indicate that removal of the bone block of the patella alters the biomechanics of the kneecap which could lead to earlier arthritis of the kneecap joint. Finally, the early rehabilitation process can be painful because it is required that the patient bend their knee to regain motion even after they have had bone and patella tendon removed. There is also an early risk of fracture of the patella because it is temporarily weaker from the bone harvest. Therefore, a patient must not increase their activity too aggressively early on in the rehabilitation process.